
Montreal, December 2nd 2022
Author: Dr. W. Kowalski, Chief Scientist, Sanuvox Technologies Inc.
Sanuvox Technical Report
Schools, especially grade schools, kindergartens and daycare facilities, are focal points for disseminating airborne diseases to the rest of society. The pattern of children bringing viruses and other pathogens home to infect their siblings and their parents has remained unchanged since it was first recognized in the 1930s.
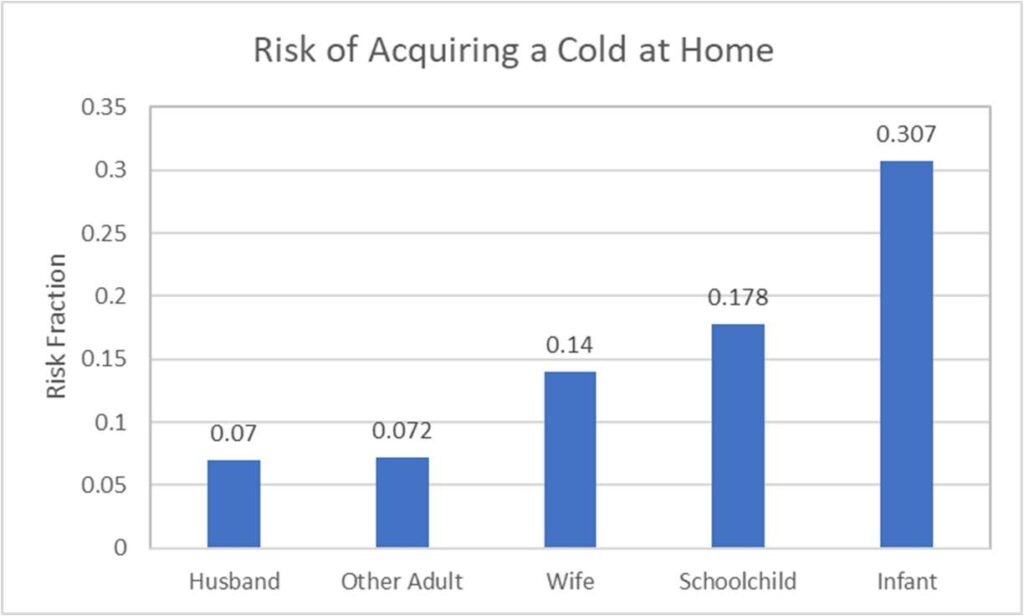
Recently, in the wake of COVID-19, outbreaks of a cocktail of viruses, including RSV and Rhinoviruses, have spread across the country, presumably taking advantage of the reduced immunity that would have been conferred by each of these viruses had they been acquired separately and sporadically over the 2-year course of the coronavirus pandemic. Considering that schools are probably the number one source that is radiating contagious infections to the public, it is surprising how little attention is placed on solving the problem of disease dissemination in schools. Figure 1 illustrates the risk of acquiring a cold at home. Although infants are most susceptible, it is likely that the school child first brings the virus home from school.
Among different types of buildings, classrooms have the highest average bacteria and fungi levels (Guo 2020). Studies show that the concentration of indoor bacteria varies from 72.5 to 7500 CFU/m3, with a median value of 1000 CFU/m3, and the concentration of fungi varies from 12 to 9730 CFU/m3, with a median value of 526 CFU/m3. Air sampling for viruses is problematic, but it can be reasonably inferred that airborne levels of viruses are also highest in schools.
Hygiene may be the biggest problem for children in schools. A review of curriculums in kindergarten and grade schools reveals that Hygiene is not a standard subject, and though children are taught numbers, letters and even how to count the money, they are not taught how to protect themselves from contagious viruses. Hygiene should be the first and most important subject taught to children today. Handwashing, for example, is one of the most critical factors in controlling the spread of micro-organisms and can reduce infections by over 50% (Guinan 2002). Quarantine is another measure that can protect students, but it is little utilized – sick students are often sent home where the infection they picked up at school will spread to family members.
After hygiene, the next best strategy is air cleaning technology. The air exchange rate in schools can be increased to try to lower infection rates. Air filtration can be useful for removing large spores or bacteria, but attempting to remove viruses from the air with just filtration is cost-prohibitive (Kowalski 2021). Regular cleaning of school surfaces with detergents or disinfectants can go a long way towards protecting occupants. Ultraviolet
technology for cleaning the air and surfaces in schools can minimize the transfer of new infections.
Guidelines from ASHRAE (1989) recommend homes receive no less than 0.35 air changes per hour of outdoor air, but no minimum is provided for schools. Boosting airflow in schools has been championed as one alternative for cleaning the air but making major retrofits to school building ventilation systems and boosting outside airflow in cold climates may not be the best economic choice depending on location. Airflow can also be effectively boosted by incorporating UV lamps in the ductwork of ventilation systems. This increases the effective air exchange rate, or a number of air changes per hour.
Ultraviolet light technology can be used for disinfection of air and surfaces in schools. Air can be disinfected with UV lamps placed in supply or return ductwork, and this is the most effective and economic approach for eliminating airborne viruses like coronavirus. Surface UV disinfection systems are currently in use in hospitals but these may not be as practical for schools as standard cleaning and disinfection protocols. Local UV air recirculation units, which often include filters, can provide clean air directly in the room at the source from where viruses may be disseminated, but this approach is considerably more costly than disinfecting the supply or return air.
Upper Room UV systems can also be used to disinfect classroom air but these are less effective and more costly than in-duct UV air disinfection systems. Upper Room UV systems depend on unpredictable air currents in the upper room ceiling area and also cause concerns about eye exposure to hazardous UV rays. The limited effectiveness of Upper Room UV systems can be improved by adding fans directly to the Upper Room unit or by placing fans inside the room which is being irradiated.
The first UV systems used for disinfecting air were Upper Room systems in which naked UV lamps were suspended near the ceiling in troffers that would block most harmful UV rays to the lower areas, in naturally ventilated buildings. Improved Upper Room UV systems were developed later but as more modern buildings implemented forced air ventilation it became possible to install UV lamps safely in ductwork where the full amount of building air could be disinfected economically. Such systems were never widely implemented and it is only due to the coronavirus pandemic that ventilation air disinfection systems are being considered.
The first air disinfection systems placed in schools were upper room systems (Wells 1938, Wells 1942). Table 1 summarizes the results of a number of studies in which Upper Room UV systems were placed in classrooms. Results are somewhat mixed as one might expect for systems placed in buildings without forced ventilation air or with uncertain airflows.
Table 1: Upper Room UV Field Trial Results in Schools
| Location | Infection | % Reduction of Infections | Source |
| Germantown Friends School, PA | Mumps | 82 | Wells (1938) |
| Germantown Friends School, PA | Measles | 20 | Wells (1943) |
| Germantown Friends School, PA | Cold Viruses | 18 | Wells (1943) |
| Combined Results for 4 PA Schools | Measles | 43 | Wells (1943) |
| National Training School for Boys, DC | Respiratory Infections | 0 | Schneiter (1944) |
| New York State 3-school study | Measles | 0 | Perkins (1947) |
| Mexico, Cato-Meridian & Port Byron schools | Chicken Pox | 25 | Bahlke (1949) |
| Southall Elementary Schools, England | Measles | 14 | MRC (1954) |
| Southall Elementary Schools, England | Mumps | 61 | MRC (1954) |
| Southall Elementary Schools, England | Chicken Pox | 17 | MRC (1954) |
| Mexico & Cato-Meridian schools | Mumps | 75 | Wells (1955) |
| Port Byron School | Mumps | 6 | Wells (1955) |
The results shown in Table 1 are for Upper Room UV systems that had no integral fans and for which no fans existed in the room itself. Certainly, results would be improved with modern Upper Room systems with built-in fans or that are augmented with room fans. Although there are no studies in schools, one could speculate that forced air UV disinfection systems would have produced improved results that are probably maximized in any schools that have dedicated ventilation systems.
In conclusion, ultraviolet technologies can make a difference in reducing infectious disease transmission in schools when they are properly selected, designed and implemented. Forced air UV disinfection is the most effective and economical approach to reducing indoor levels of pathogenic microorganisms in schools. In naturally ventilated buildings where air exchange rates are minimal or uncertain, Upper Room UV systems can provide an economic expedient but without the guaranteed performance of a dedicated UV ventilation air disinfection system. Local UV recirculation units can also be effective but are the most expensive alternative.
References
ASHRAE (1989). Standard 62R: Ventilation for acceptable indoor air quality, ASHRAE.
Bahlke, A. M., et al. (1949). “Effect of ultra-violet irradiation of classrooms on spread of mumps and chickenpox in large rural central schools.” Am J Pub Health 41: 1321-1330.
Gelperin, A., et al. (1951). “The Effect of Ultraviolet Light upon Absenteeism from Upper Respiratory Infections in New Haven Schools.” Am J Pub Health 41: 796-805.
Guinan, M., et al. (2002). “The effect of a comprehensive handwashing program on absenteeism in elementary schools.” Am J Infect Control 30(4): 217-220.
Guo, K., et al. (2020). “Indoor exposure levels of bacteria and fungi in residences, schools, and offices in China: A systematic review.” Indoor Air 30(6): 1147-1165.
Kowalski, W., D. Saputa, D. Jones. (2021). “Achieving MERV-13: UV-C Can Help Less Efficient HVAC Filters Get There.” HPAC Engineering 93(6): 38-44.
Lidwell, O. M. and R.E.O.Williams (1961). “The epidemiology of the common cold.” Journal of Hygiene 59: 309-334.
MRC (1954). Air Disinfection with Ultra-violet Irradiation; Its Effect on Illness among School-children by the Air Hygiene Committee. London, Medical Research Council, Her Majesty’s Stationary Office.
Perkins, J. E., et al. (1947). “Effect of ultra-violet irradiation of classrooms on the spread of measles in large rural central schools.” Am J Pub Health 37: 529-537.
Schneiter, R., A. Hollaender, B. H. Caminita, R. W. Kolb, H. F. Fraser, H. G. duBuy, P. A. Neal and H. G. Rosenblum (1944). “Effectiveness of ultra-violet irradiation of upper air for the control of bacterial air contamination in sleeping quarters.” Am J Hyg 40: 136.
Wells, W. F. (1943). “Air Disinfection in Day Schools.” Am J Public Health Nations Health 33(12): 1436-1443.
Wells, W. F. (1938). “Air-borne infections.” Mod Hosp 51: 66-69.
Wells, W. F., et al. (1942). “The environmental control of epidemic contagion; I – An epidemiologic study of radiant disinfection of air in day schools.” Am J Hyg 35: 97-121.
Wells, W. (1955). Airborne Contagion. New York, New York Academy of Sciences.